
Concussion Remission and CTE – Part 1
“I believe it is medical malpractice not to offer [HBOT] to our Veterans.” Congressman Greg Murphy (R-NC)
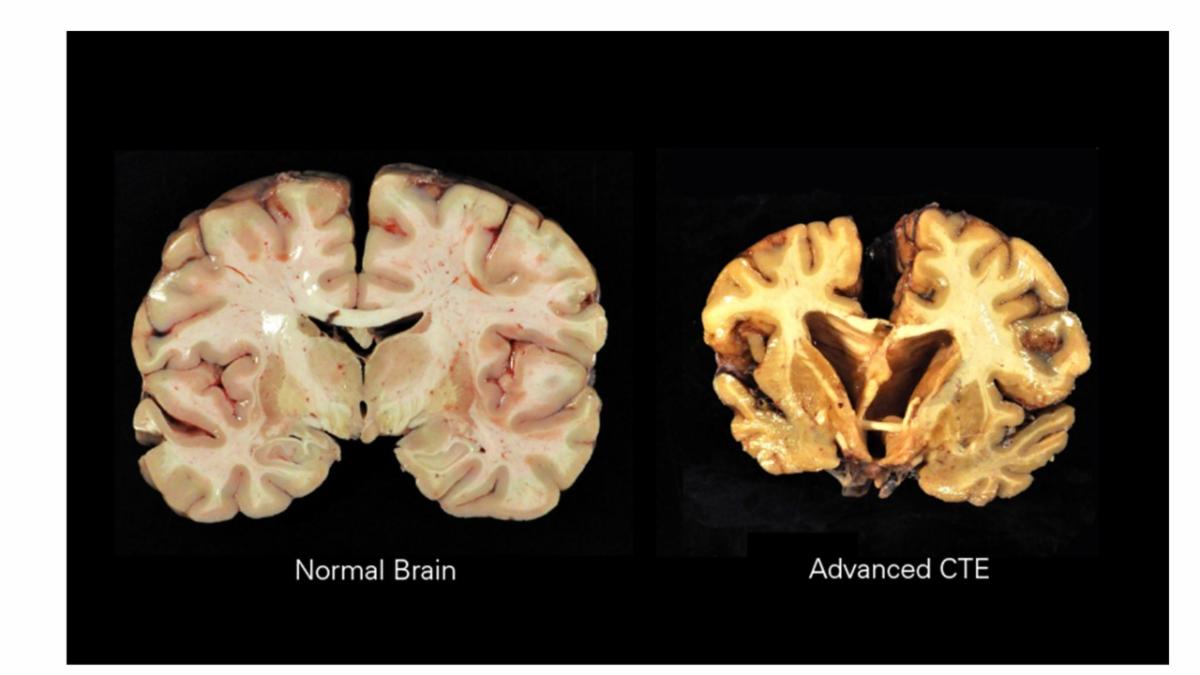
“Deja vu all over again.” Chronic Traumatic Encephalopathy (CTE) and Concussion research and reporting is following a well-worn path that leads to lots of money for research, billions of written words in thousands of studies — and untold numbers of avoidable deaths.
A man slaughters people in New York and the NFL Commissioner offers thoughts and prayers. Reporters and social media race to determine why the kid complained about CTE? The usual medical suspects are interviewed and report that we just don’t know yet it he had CTE, or even whether CTE was the cause of his behavior and death. Could we, should we, have done more earlier to head off the slaughter?
Imagine if we lived in a world where a treatment for a disease was known to work, where that treatment was used successfully worldwide to treat that disease, and the U.S. medical community continued to drag its feet and not use the treatment. It’s happened before.
1932-1972. For forty years, the Tuskegee Syphilis Study was designed to to observe the natural history of untreated syphilis, despite a cure being widely available by 1945. Penicillin was so widely recognized as a cure for syphillis that the Nobel Prize was awarded in 1945 to Fleming, Chain and Florey. They received the award for their “discovery of penicillin and its curative effect on various infectious diseases”. Millions of doses were available by D-Day and penicillin was widely available to the public by 1946. Still the Tuskegee researchers withheld it from study participants, all the way until 1972 when the study was exposed and ended. No one was prosecuted; no one went to jail.
The Tuskegee Study violated several fundamental ethical principles of research, primarily involving informed consent, beneficence, and justice. Participants were not adequately informed about the nature of the study, the risks involved, or the availability of effective treatment (penicillin). This lack of informed consent meant they were not able to make a truly voluntary decision to participate. The study also failed to act in the best interests of the participants by withholding treatment, which led to unnecessary suffering and death.
Jump shift to 2025. The CDC reports that millions of Americans are suffering from diagnosed and undiagnosed brain injuries. There are around 2.8 million TBI-related emergency department visits, hospitalizations, and deaths each year. An estimated 5.3 million Americans are currently living with a TBI-related disability, and roughly 15% of them — 795,000 — experience long-term disabilities or neurological issues. More than 56,000 deaths annually are attributed to TBI. Over 153,000 service members have succumbed to suicide since 9/11, too many with undiagnosed brain wounds.
Now consider the superstructure in place to guide this multibillion dollar enterprise. Start with how many names we have for “concussion.” Concussion, Mild Traumatic Brain Injury (m)TBI, Traumatic Brain Injury (TBI), Closed/Open Head Injury, Diffuse Axonal Injury (DAI), Coup-Contrecoup Injury, Brain Contusion, Invisible Wounds of War, Blast-induced TBI, Post-Concussive Syndrome, Second impact Syndrome, Post Traumatic Stress Disorder (PTSD), Operator Syndrome, Polytrauma, CTE (Chronic Traumatic Encephalopathy), and Traumatic Encephalopathy Syndrome (TES).
A search of Centers Excellence to treat Concussion turns up several Centers of Excellence focused on concussion and traumatic brain injury (TBI) within the U.S. military and the VA healthcare system. The Traumatic Brain Injury Center of Excellence (TBICoE) is a key organization, supporting a multi-center network of military and VA facilities. Additionally, the National Intrepid Center of Excellence (NICoE) serves as the headquarters for the 13-site Defense Intrepid Network for TBI and Brain Health, which includes several Intrepid Spirit Centers. There are also 87 Polytrauma Support Clinic Teams (PSCT) within VA medical centers that provide specialized concussion care.
That’s in the military system. The U.S. healthcare sector employs over 17 million people, making it the largest employment sector in the country. Over one million are Mental Health professionals. They work in over 12,000 facilities. Across the US, there are thousands of facilities in the US dealing with management of Concussion. Large hospital systems and academic medical centers like the Mayo Clinic, Cleveland Clinic, and NYU Langone; Sports medicine and orthopedic clinics; Private rehabilitation centers; and Outpatient therapy networks that offer concussion rehab as part of their neuro rehab programs.
Research includes the world’s largest longitudinal study of Concussion administered at Indiana University. The CARE Consortium is a global, multi-institutional study involving over 53,000 collegiate athletes and military cadets. It is not a clinical study, but researchers have discovered that “80% [of concussed athletes] took up to four weeks to recover while the vast majority of the remaining 20% were able to return to play if given an additional month to recover.” Weeks and months to get to where they can pass a Return to Play test. Not because they are healed, but because they can pass a test. And data collection continues, but no advice to the wounded to try healing with HBOT.
We as a nation have built a similar superstructure to create “Suicide Prevention” strategies. Billions of dollars spent alongside a continuing increase in the suicide epidemic with barely a question: “Can’t we do SOMEthing differently that could work?” Should we add to the $5 Billion already spent by the CDC, HHS, VA, DOD, NIH and other government agencies, only to watch the suicide epidemic continue to rise? Can’t we improve the way we treat brain wounds to reverse the misery and death?
You’ll search in vain for any mention of healing brain wounds.
Look at any of a dozen professional sports Concussion Protocols: the NFL; FIFA; the NCAA; the NHL; the RUGBY LEAGUE; MAJOR LEAGUE SOCCER; the NBA; MLB; the OLYMPIC COMMITTEE; the WNBA; WOMEN’S MAJOR LEAGUE SOCCER; or the EUROPEAN LEAGUE. Not one mention of a brain wound. Nor of the word “oxygen.” They are all focused on diagnosis and return-to-play, without taking the time to discuss TREATMENT of the brain wound. They talk of “management” of symptoms. They search for new drugs, but ignore the one drug the brain craves: oxygen.
If we managed well-known athletic injuries the way we manage Concussion, we’d wait around and hope an ACL tear or broken bones healed themselves. Just because an “invisible wound” like concussion can’t be seen, doesn’t mean that it can’t be treated like the wound that it is. And decades of peer-reviewed research and tens of thousands of successes worldwide back up that claim.
So why, after two decades of published research and positive findings about safety and efficacy, do we not employ Hyperbaric Oxygen Therapy to Concussions, AKA mild traumatic brain injury?
It is a well-known phenomenon that failing organizations spend more time and money “admiring the problem” than solving it. And the crowd around the Concussion Protocol is a failing organization. Untold sums are spent on naming, diagnosing, photographing, rehabbing, and NOT treating concussions than are spent on root-cause-analysis and resolution of the problem: a brain wound, untreated, is a continuing disease state, perhaps for life.
Veterans and athletes and ordinary citizens are part of a long-running study whose results are already known, but a known effective drug is not being used to help heal their brain wounds. Oxygen under pressure is that drug and Part Two explores the myths and realities of Hyperbaric Oxygen Therapy, the “concussion cascade,” and why Congressman Murphy is right to assert that we as a society are guilty of medical malpractice for not using a proven therapy to heal concussions: HBOT. Heal Brains. Stop Suicides. Restore Lives. Change Medicine.
******************************
The TreatNOW Mission is ending service member suicides. Along the way, we have learned that we can end suicidal ideation, help end symptoms of PTSD, get patients off most of their drugs, and heal brain wounds to end the effects of Concussion, BLAST injury, mild TBI Persistent Post Concussive Syndrome, and polytrauma from AHI, Burn Pits, and COVID. No Veteran or civilian has ever been killed while undergoing HBOT treatment for TBI/PTSD. For a video Summary, see: https://www.youtube.com/@treatnowdotorg/videos
Information provided by TreatNOW.org does not constitute a medical recommendation. It is intended for informational purposes only, and no claims, either real or implied, are being made.
